
Pulmonary Medicine Blog By Dr Deepu















Bronchiectasis is an abnormal and permanent distortion of one
or more of the conducting bronchi or airways.


Types of bronchiectasis

Cylindrical Bronchiectasis
Mild Form shows Tram Track Appearance


Varicose Bronchiectasis
Moderate Form appears as string of pearls

Cystic/ Saccular Bronchiectasis
Severe Form appears like Bunch of Grapes

Chest
radiography Chest radiography (CXR) is usually the initial study performed in
both suspected bronchiectasis and the evaluation of nonspecific respiratory
symptoms, such as dyspnoea and haemoptysis, when bronchiectasis may be
identified incidentally.
Signs on CXR are the
identification of
Read This X Ray Before Proceeding Further
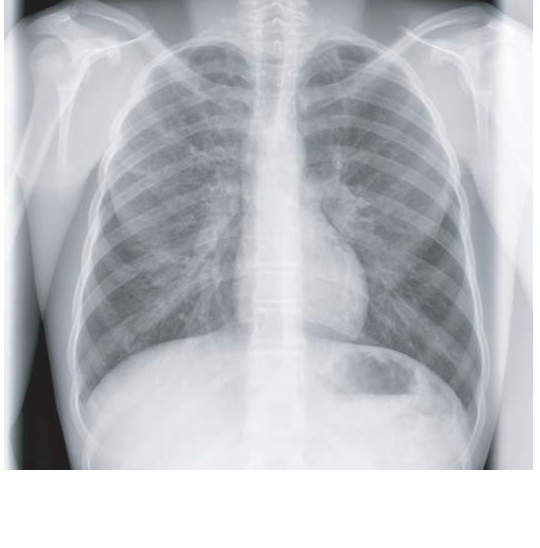
1. Parallel
linear densities, tram-track opacities.
what was seen on the chest X ray, it is nothing but the tram line appearance, unable to spot it, here comes the Modified image

Now Compare the previous X Ray with the one above , Here are few examples of tram line shadows


The black arrows points towards tram line and the white to shadows which will be discussed below
Read this X ray before proceeding

What Can we see here
if you have got it proceed further

What we see here is the ring shadows, there are many other ring shadows in the x ray , only a few are marked
One More X ray below showing the ring shadows in Cystic Fibrosis Patient


2. Ring
shadows reflecting thickened and abnormally dilated bronchial walls. These
bronchial abnormalities may vary from subtle
or barely perceptible 5-mm ring shadows to obvious cysts.
3. Fluid or mucous filling of bronchi is seen and
leads to Tubular branching opacities conforming to the expected bronchial branching
pattern.




4. The Definition
of vessel walls is lost due to peribronchial
fibrosis.
5. Signs
of complications/exacerbations, such as patchy densities due to mucoid
impaction and consolidation
6. Volume loss secondary to bronchial mucoid
obstruction or chronic cicatrisation, are also seen.
7. In the
more diffuse forms , such as cystic fibrosis (CF), generalised hyperinflation
and oligaemia are often present, consistent with severe small airways
obstruction.
The radiograph may raise the initial suspicion of
bronchiectasis, triggering more definitive imaging.
CXR also plays a role in the follow-up of bronchiectasis and management of exacerbations.Although CXR has limitations in specificity in diagnosing bronchiectasis and in detecting early or subtle changes, it is useful for assessing more florid cases of bronchiectasis, in CF and in follow-up of bronchiectatic patients. Computed tomography.
suggested Reading
CXR also plays a role in the follow-up of bronchiectasis and management of exacerbations.Although CXR has limitations in specificity in diagnosing bronchiectasis and in detecting early or subtle changes, it is useful for assessing more florid cases of bronchiectasis, in CF and in follow-up of bronchiectatic patients. Computed tomography.
suggested Reading















.jpg)








