
Showing posts with label chest x ray. Show all posts
Showing posts with label chest x ray. Show all posts
Tin Man Syndromes or Ectopia cordis Interna
By Dr Deepu
The following case was reported by Dr Matt Skalski in radiopedia.The chest X ray was done on a person for employment screeing. The chest X ray showed no heart. Rare isn't it. On enquiry he didnt have any symptoms other than gastric reflux. Then a CT was done which showed heart inside the stomach.
This was the X ray picture



This condition is called as Tin Man syndrome or Ectopia cardiac internalis, meaning heart is present at a different site inside the body.
Let us have a look at the CT films of the abdomen.






The CT images shows heart in the abdomen.
Now let's know the historical aspects of TIN MAN syndrome which is extremely rare.

This picture is of Da Vincis organ newotks of
the thoracoabdominal cavity.There remains debate as to whether Leonardo Da
Vinci's "Organ networks of the thoracoabdominal cavity"
illustration (c.1502) was based off a corpse with ectopia cordis
interna, or whether his depiction of the heart's location was a
deliberate distortion of reality. Most legitimate scholars believe Da
Vinci created the work as a flight of anatomical
fancy.
The first ever description of the condition in
the medical literature was in a controversial
monograph submitted to the Royal Society in 1874 by Dr.
Nohear Lubdub. Entitled "An unusual case of ectopia cardia
epigasticum in a Haryana boy", the monograph was later retracted when
accusations were made that the images accompanying the text had been
doctored.
It was not until 1908 that Dr Lubdub's work was
vindicated when existence of the condition was confirmed during
the early years of chest radiography. Unfortunately,
Dr Lubdub had fallen into a deep depression following his expulsion
from the Royal Society, only occasionally seen wandering the streets
of Chandigarh mumbling "and yet it beats". His death
was unrecorded.
Disclaimer : this was a April Fool Case published in Radiopedia.org and is Imaginary.
Disclaimer : this was a April Fool Case published in Radiopedia.org and is Imaginary.
Case courtesy of Dr Matt Skalski,
Radiopaedia.org.
From the case rID: 33437
Signs in chest radiology- The hilum overlay sign
By Dr Deepu


The hilar overlay sign is another sign described
by Felson.The
hilum overlay sign refers to an appearance on frontal chest X ray of patients
with a mass at the level of the hilum which is in fact either anterior or
posterior to the hilum.



When
a mass arises from the hilum, the pulmonary vessels will be in contact with the
mass and hence their silhouette is obliterated. The ability to see and trace
the edges of the vessels through the mass implies that the mass is not
contacting the hilum, and is therefore either anterior or posterior to it.

want to read more in chest radiology??? Have a look at the following pages
Signs in chest radiology- The silhouette Sign
By Dr Deepu
Silhouette sign/loss of silhouette sign/ loss of
outline sign.
I was always confused with the silhouette sign for
its hidden meaning and failure to decode it by many medical students. So, I
thought it would be apt to unravel it so that it could be handy for many
medical students.
One of the most useful signs in chest radiology is
the silhouette sign. This sign was described by Dr. Ben Felson. The silhouette
sign is in nothing but elimination of
the silhouette or loss of lung/soft tissue interface caused by a mass or fluid
in the normally air filled lung. For instance, if an intrathoracic opacity is
in anatomic contact with, for example, the heart border, then the opacity will
obscure that border. The sign is commonly applied to the heart, aorta, chest
wall, and diaphragm. The location of this abnormality can help to determine the
location anatomically.
Just go through the X Ray to know the various structures seen in the chest x ray.

Let me explain this with this image.
What do we see???
There is plastic bottle which is surrounded by air,
the margins of the shadow is very well
demarcated from the surrounding air.

First scenario: There are two bottles, made of same
material, placed apart from each other. The shadows appears separate from each
other. Let us consider the right bottle to be the heart and the air surrounding
the bottle as lung. The left bottle as a mass, since they are far from each
other, the border of both is visible
clearly.

Second scenario: Here we see the bottles are
touching each other at two points and there is no gap in between and if we look
at the shadow, we cannot differentiate between the two shadows, they appear
like a single opacity at the upper and lower ends.

For the heart, the silhouette sign can be caused by
an opacity in the RML, lingula, anterior segment of the upper lobe, lower
aspect of the oblique fissure, anterior mediastinum, and anterior portion of
the pleural cavity.
This
contrasts with an opacity in the posterior pleural cavity, posterior
mediastinum, of lower lobes which cause an overlap and not an obliteration of
the heart border. Therefore both the presence and absence of this sign is
useful in the localization of pathology.
want to read more in chest radiology??? Have a look at the following pages
Chest Radiology
Signs in Chest Radiology
want to read more in chest radiology??? Have a look at the following pages
Chest Radiology
Signs in Chest Radiology
signs in chest radiology Bulging Fissure Sign
By Dr Deepu


Bulging
Fissure Sign


The
bulging fissure sign, it represents expansive lobar consolidation causing
fissural bulging or displacement by copious amounts of inflammatory exudate
within the affected parenchyma, seen in a chest x ray. It is classically associated with right upper
lobe consolidation due to Klebsiella pneumoniae , any form of pneumonia can
manifest the bulging fissure sign. The
prevalence of this sign is decreasing,because of prompt administration of
antibiotic therapy to patients with suspected pneumonia . The bulging fissure
sign is also less commonly detected in patients with hospital-acquired
Klebsiella pneumonia than in those with community-acquired Klebsiella infection
.
Other
diseases that manifest a bulging fissure
any space-occupying process in the lung, such
as
pulmonary
hemorrhage,
lung abscess, and
tumor
want to read more in chest radiology??? Have a look at the following pages
Plombage - An Obsolete Technique of Historical Importance in treating TB
By Dr Deepu
 |
| Chest X Ray of Plombage using Lucite Balls |
 |
| CT Thorax of the same Patient |
Plombage was a surgical method used prior to the introduction of anti-tuberculosis drug therapy to treat cavitary tuberculosis of the upper lobe of the lung. The term derives from the Latin word "plumbum" (lead) and refers to the insertion of an inert substance in the pleural space. The technical medical term for plombage is extraperiosteal or extrapleural pneumonolysis.
The underlying theory of plombage treatment was the belief that if the diseased lobe of the lung was physically forced to collapse, it would heal quickly. There were positive results in tuberculosis therapy following plombage in the decades of the 1930s, 40s and early-50s. However, with the introduction of drugs which were effective in destroying the tuberculosis bacterium (Mycobacterium tuberculosis), plombage treatment fell into disfavor. In addition, complications of plombage began to appear in patients who had been so treated. These complications included hemorrhage, infection and fistulization of the bronchus, aorta, esophagus and skin.
The technique involved surgically creating a cavity underneath the ribs in the upper part of the chest wall and filling this space with some inert material. A variety of substances were typically used and included air, olive or mineral oil, gauze, paraffin wax, rubber sheeting or bags and Lucite balls. The inserted material would force the upper lobe of the lung to collapse.
NEJM LINKS FOR LUCITE BALLS

MELTING ICE(CUBE) SIGN
By Dr Deepu

The melting ice(cube) sign describes the resolution of. pulmonary haemorrhage following pulmonary embolism.
When there is pulmonary haemorrhage without infarction following PE, the typical wedge-shaped, pleural-based opacification (Hamptons Hump) resolves within a week while preserving its typical shape. It is named due to its resemblance with a melting ice cube.
1. Webb WR, Higgins CB. Thoracic Imaging: Pulmonary and Cardiovascular Radiology, North American Edition. Lippincott Williams & Wilkins. (2010) ISBN:1605479764.
Suggested Reading
1. Chest X Ray Part 1- Normal Anatomy And ItsVariants

The melting ice(cube) sign describes the resolution of. pulmonary haemorrhage following pulmonary embolism.
When there is pulmonary haemorrhage without infarction following PE, the typical wedge-shaped, pleural-based opacification (Hamptons Hump) resolves within a week while preserving its typical shape. It is named due to its resemblance with a melting ice cube.
1. Webb WR, Higgins CB. Thoracic Imaging: Pulmonary and Cardiovascular Radiology, North American Edition. Lippincott Williams & Wilkins. (2010) ISBN:1605479764.
Suggested Reading
1. Chest X Ray Part 1- Normal Anatomy And ItsVariants
SPOTTER : GIVE YOUR DIAGNOSIS
Pulmonary Medicine Blog By Dr Deepu
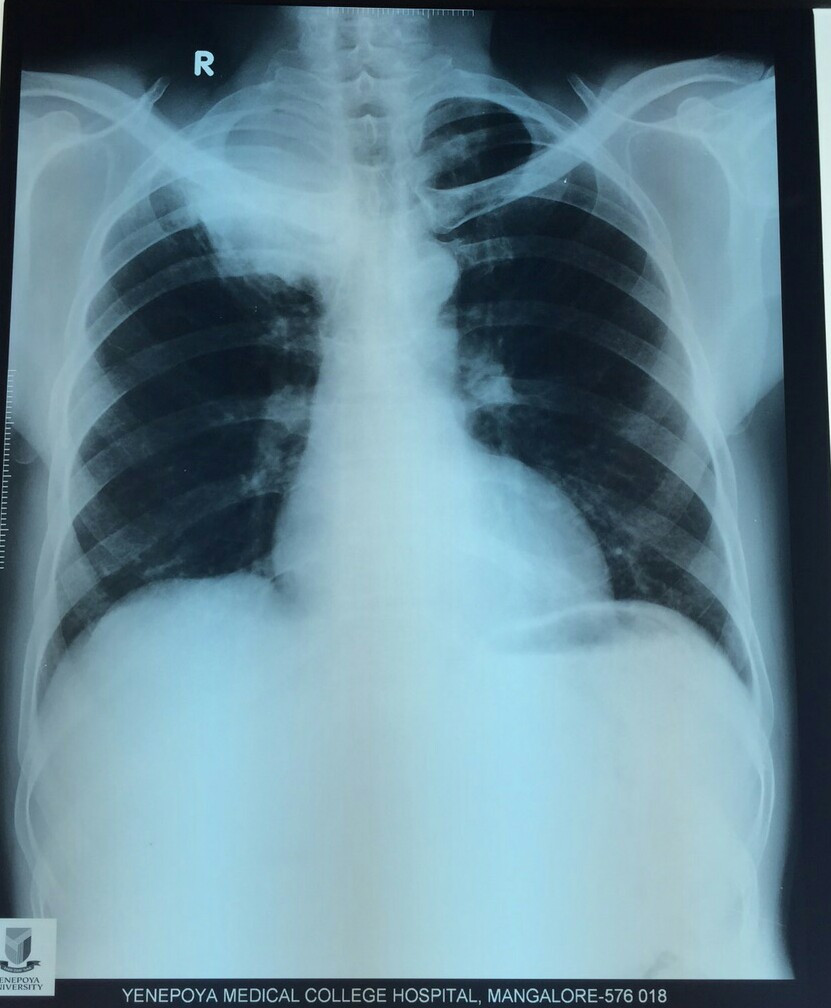
Mr X came to the out patient department with hemoptysis since 2 weeks, and chest pain in the right upper part anteriorly since 2 weeks. On questioning he further revealed weight loss since 2 months.
Chronic smoker with 60 pack years.
Examination revealed grade 3 clubbing. Clinical examination was normal.
This Chest X ray was taken.

Mr X came to the out patient department with hemoptysis since 2 weeks, and chest pain in the right upper part anteriorly since 2 weeks. On questioning he further revealed weight loss since 2 months.
Chronic smoker with 60 pack years.
Examination revealed grade 3 clubbing. Clinical examination was normal.
This Chest X ray was taken.
Grand Rounds - Opaque hemithorax.
Pulmonary Medicine Blog By Dr Deepu

Grand Rounds:
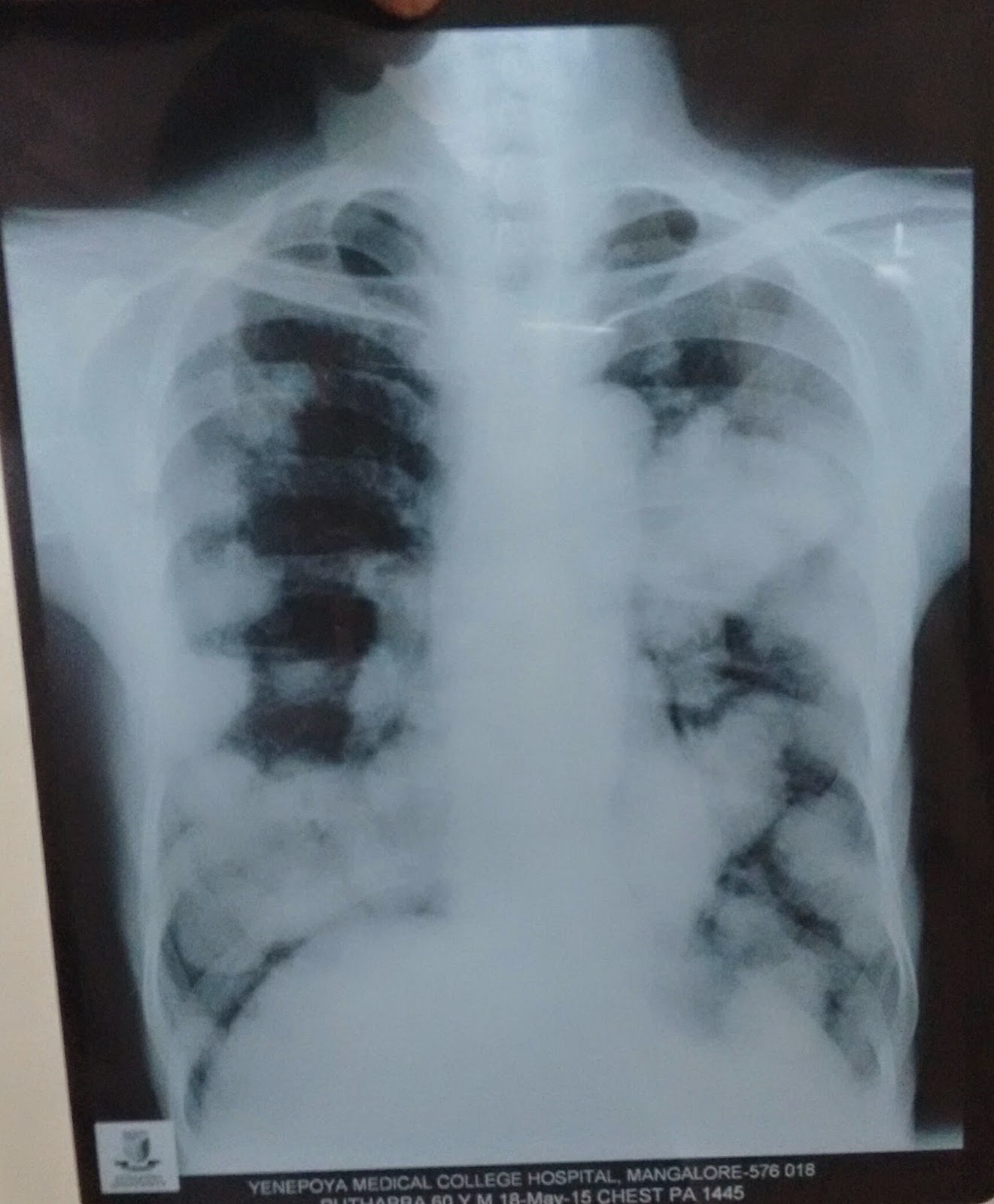
This patient an elderly lady presented to us with breathlessness and cough eith sputum with increased sputum in right lateral position. Spo2 was 89%
Examination revealed trachea deviated to left. Apicak impulse felt in left axilla 5th Ics. Breath sounds diminished on left with added crepitations on left side.
This X ray was taken in emergency room.

CT confirmed fibrosis of left lung.
Complete white out(opacification) of the hemithorax on CXR has a limited number of causes.
The differential diagnosis can be zeroed on with one simple observation - the position of the trachea.
Is it central, pulled or pushed from the side of opacification?
- pulled trachea : pneumonectomy, total lung collapse, pulmonary fibrosis,pulmonary agenesis
- central: consolidation, mesothelioma, collapse with effusion. Lung mass
- pushed: pleural effusion, diaphragmatic hernia.
Radiology- chest X Ray Spotters.
Pulmonary Medicine Blog By Dr Deepu
spotter 1.
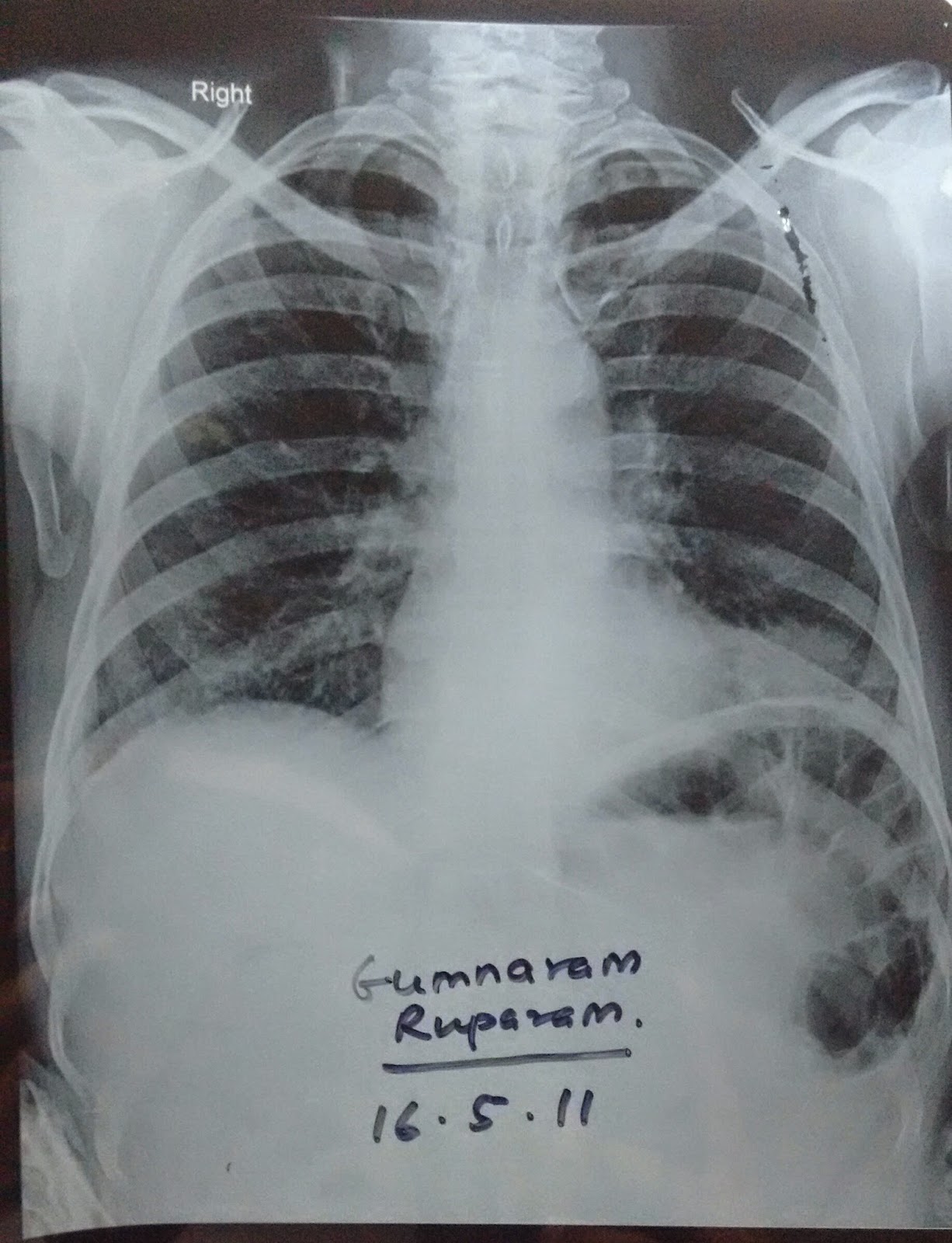
A middle Aged male who is HIV+ presents with a cough of 3 months and cachexia. Auscultation reveals crepitations b/l . Differentials???

spotter 1.
A middle Aged male who is HIV+ presents with a cough of 3 months and cachexia. Auscultation reveals crepitations b/l . Differentials???

Clinical Case - Give Your Diagnosis!!!
Pulmonary Medicine Blog By Dr Deepu
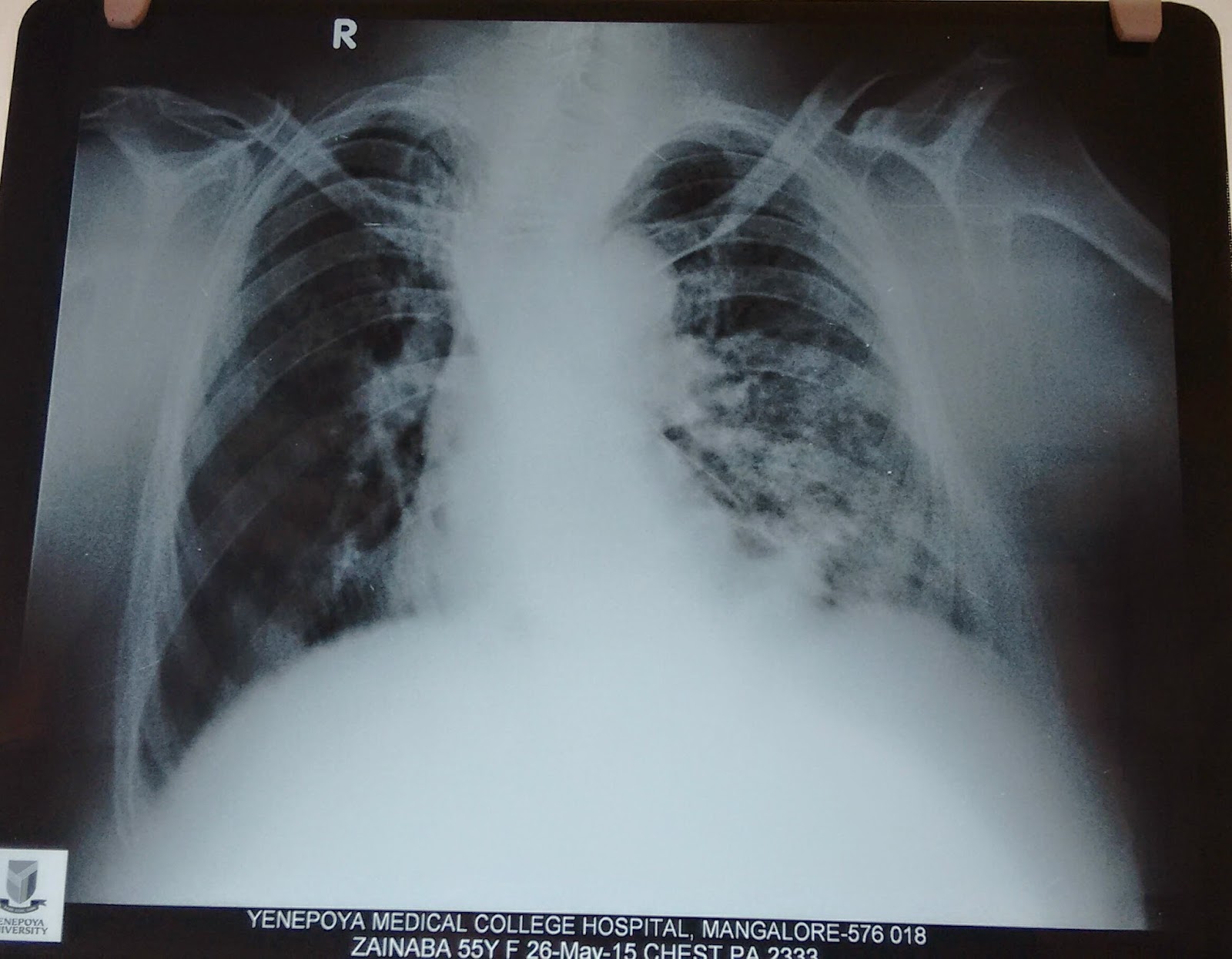
 An elderly female came to the outpatient department with a history of cough since 2 weeks minimally productive sputum, she also give history of increased breathlessness since 3 weeks, the symptom of breathlessness being present since three years, she also complains of decreased sleep due to productive cough, and a known hypertensive since 5 years.
An elderly female came to the outpatient department with a history of cough since 2 weeks minimally productive sputum, she also give history of increased breathlessness since 3 weeks, the symptom of breathlessness being present since three years, she also complains of decreased sleep due to productive cough, and a known hypertensive since 5 years.
Clinical examination reveals pitting pedal edema and bilateral basal crepitations and no other significant clinical findings were present.
Investigations revealed a total count of 13000 and this chest x ray. EKG was normal. What could be the differential diagnosis????
Clinical examination reveals pitting pedal edema and bilateral basal crepitations and no other significant clinical findings were present.
Investigations revealed a total count of 13000 and this chest x ray. EKG was normal. What could be the differential diagnosis????
Spotter : Identify the radiological sign in chest X ray.
Chest X Ray- The Diaphragm is unique and provides clue to your diagnosis!!!
Pulmonary Medicine Blog By Dr Deepu


There are a few things which
beginners often miss in a chest x ray, one among those is failure to comment on
the diaphragms.
Today I am going to discuss
importance of tracing diaphragm in a chest X ray with an example.
Normal diaphragm in a chest X ray has
the following characteristics


1. Trace
the diaphragm on right and left
2. The right
diaphragm is usually placed between the fifth and the sixth Rib in the mid
clavicular line, It can be seen upto middle of sixth and seventh rib.
3. The
Diaphragms are usually not at the same level on the frontal , erect ,
inspiratory chest X rays, but they are usually within one rib intercostals space
height ( roughly 2 cm) of each other.
4. The
left diaphragm is usually lower than right.
5. The
costophrenic angles should be sharp, making an acute angle.
6. If the left hemidiaphragm is equal to Right or
higher than Right or Right diaphragm is higher than left by more than 3 cms,
Causes of diaphragmatic elevation should be considered.
The causes of elevated hemidiaphragm are
1.
Causes above the diaphragm- decreased lung
volume due to Lung Collapse, lobectomy, pneumonectomy , fibrosis and pulmonary
Hypoplasia
2.
Causes in the diaphragm- Phrenic nerve palsy ,
diaphragmatic evantration
3.
Causes below the diaphragm- abdominal
malignancy, subphrenic abscess, distended hollow
viscus.
After knowing the cause I want to discuss
with you a chest x ray where the subtle change in the diaphragm was missed.
Before we proceed Read the chest X ray
The Chest X ray showed a subtle change in Diaphragm
1. Both the diaphragms are at the same levels.
2. The air shadow underneath the left diaphragm is more prominent.
3. The patient was not evaluated further because chest X Ray appeared normal and sent home with conservative treatment for COPD.
He came back to our center with hemoptysis one month later referred from the center which treated him initially, a second Radiograph was performed. study the Chest X Ray before proceeding further.
The chest X ray now shows features of full blown disease, the hilum is prominent with CORONA RADIATA SIGN suggestive of bronchogenic carcinoma, The left Diaphragm is now placed higher compared to right. Further HR and CECT revealed a tumor in the Left Main bronchus with lymph node metastasis. With Bronchoscopy the diagnosis of squamous cell carcinoma was made.
With this I will end this post, requesting everyone to look at any subtle changes in diaphragm which if ignored may cause some grave diagnosis at a later date.
Basics Of Chest X Ray Part-6, The Lungs, Pleura And The Chest Wall.
Pulmonary Medicine Blog By Dr Deepu















.jpg)









Lung
abnormalities mostly present as areas of increased density, which can be divided
into the following patterns:
Consolidation
Atelectasis
Nodule or
mass - solitary or multiple
Interstitial
Less
frequently areas of decreased density are seen as in emphysema or lungcysts.
BEST BOOK FOR CHEST RADIOLOGY
BEST BOOK FOR CHEST RADIOLOGY
Chest X-Ray - Lung disease.
Consolidation
Atelectasis
Nodule
- Masses
Solitary
pulmonary node
Interstitial
pattern
Interstitial
lung diseases will be discussed in coming posts.
Pleura
Pleural
fluid
It
takes about 200-300 ml of fluid before it comes visible on an CXR (figure).
About 5
liters of pleural fluid are present when there is total opacification of the
hemithorax.
Total
opacification of the right hemithorax in a patient with pleuritis carcinomatosa
on both sides.
SUGGESTED BOOKS
SUGGESTED BOOKS
On the
right there is only some air visible in the major bronchi creating an air
bronchogram within the compressed lung.
Pleural
fluid may become encysted.
Here we
see fluid entrapped within the fissure.
This
can sometimes give the impression of a mass and is called 'vanishing tumor'.
Pneumothorax
The
table lists the most common causes of a pneumothorax.
The
other cystic lungdisease which causes pneumothorax is Langerhans cell
histiocytosis (LCH) which is seen in smokers.
Study
the CXR.
There
are two important findings.
The
retracted visceral pleura is seen (blue arrow) which indicates that there is a
pneumothorax.
There
is a horizontal line visible (yellow arrow).
Normally
there are no straight lines in the human body unless when there is an air-fluid
level.
This
means that there is a hydro-pneumothorax.
When a
pneumothorax is small, this air-fluid level can be the only key to the
diagnosis of a pneumothorax.
Study
the CXR.
There
are 3 important findings.
Notice
that the mediastinum is slightly displaced to the left.
Does
this mean that there is a tension pneumothorax?
Do you
have an idea about the cause of the pneumothorax?
There
is a hydropneumothorax.
Notice
the air-fluid level (blue arrow).
The
upper lobe is still attached to the chest wall by adhesions.
Maybe
this patient was treated for a prior pneumothorax.
There
is a lung cyst in the upper lobe (red arrow).
So we
can assume that the pneumothorax has something to do with a cystic lung
disease.
Since
this patient is a woman, lymphangioleiomyomatosis (LAM) is a possible
diagnosis.
LAM is
a rare lung disease that results in a proliferation of smooth muscle throughout
the lungs resulting in the obstruction of small airways leading to pulmonary
cyst formation and pneumothorax.
LAM
also occurs in patients who have tuberous sclerosis.
Study
the CXR.
What is
your diagnosis?
This is
not a pneumothorax but a skin fold.
The
radiography was performed supine with a CR cassette inserted underneath the
patient, which resulted in a skinfold.
Notice
that there are lung markings beyond the apparent pneumothorax.
Here
two CXRs of another patient with obvious skinfolds.
Recognition
of a pneumothorax depends on the volume of air in the pleural space and the
position of the body.
On a
supine radiograph a pneumothorax can be subtle and approximately 30% of
pneumothoraces are undetected.
A sign
to look for is the 'deep sulcus sign'.
It
represents lucency of the lateral costophrenic angle extending toward the
hypochondrium (Figure).
The
image is of a patient in the ICU who is on mechanical ventilation. There was an
acute exacerbation of the dyspnea.
There
is a deep sulcus sign on the left
Notice
that the left hemidiaphragm is depressed.
This is
an important finding since it indicates a tension pneumothorax.
The
image on the below is after insertion of an intercostal drain.
Notice
that the diaphragm has regained its normal appearance.
Pleural
opacities
The
table lists the most common causes of pleural opacities.
Pleural
plaques
The CXR
shows multiple opacities.
They
have irregular shapes and do not look like a lung masses or consolidations.
Some of
these opacities are clearly bordering the chest wall (red arrows).
All
these findings indicate that we are dealing asbestos related pleural plaques.
Asbestos
related pleural plaques are usually:
bilateral
and extensive.
covering
the dome of the diaphragm.
Unilateral
pleural calcifications are usually due to:
infection
(TB)
empyema
hemorrhagic
Pleural
hematoma
These
images are of a patient, who had a pleural opacity after a chest trauma.
It was
believed to be a hematoma and resolved spontaneously.
Chest
wall
Ribfractures
The
most common identified chest wall abnormalities are old ribfractures.
The CXR
shows many rib deformities due to old fractures.
When a
rib fracture heals, the callus formation may create a mass-like appearance
(blue arrow).
Sometimes
a CT is necessary to differentiate a healing fracture from a lung mass.
Notice
the large lung volume and the enlarged pulmonary vessels.
Probably
we are dealing with pulmonary arterial hypertension in a patient with COPD.
The
second most common chest wall abnormalities that we see on a CXR are metastases
in vertebral bodies and ribs.
Notice
the expansile mass in the posterior rib on the right.
Abdomen
The
most obvious finding on this CXR is free air under the diaphragm.
This
finding indicates a bowel perforation, unless when the patient had recent
abdominal surgery and there is still some air left in the abdomen, which can
stay there for several days.
There
is another subtle finding in the left upper lobe.
A
subtle density projecting over the first rib - hidden area - proved to be a
lungcarcinoma.
Here
another patient with free abdominal air.
Notice
the very thin regular line which is the diaphragm (arrow).
At
first impression one might think that this is just some plate-like atelectasis
due to poor inspiration.
Suggested reading:
Suggested reading:
Subscribe to:
Posts (Atom)