This is the fourth Post in the series Chest X Ray Interpretation. I personally suggest to read the other three posts before proceeding
1
1
Heart and Pericardium
On a chest film only the outer contours of the heart are
seen.
In many cases we can only tell whether the heart figure is
normal or enlarged and it will be difficult to say anything about the different
heart compartments.
IMPROVE YOUR X RAY READING SKILLS, BUY A BOOK
IMPROVE YOUR X RAY READING SKILLS, BUY A BOOK
However it can be helpful to know where the different compartments are situated.

Left Atrium
Most posterior
structure.
Receives blood
from the pulmonary veins that run almost horizontally towards the left atrium.
Left atrial
appendage (in purple) can sometimes be seen as a small outpouching just below
the pulmonary trunk.
Enlargement of the
left atrium results on the PA-view in outpouching of the upper heart contour on
the right and an obtuse angle between the right and left main bronchus. On the
lateral view bulging of the upper posterior contour will be seen.

Right Atrium
Receives blood
from the inferior and superior vena cava.
Enlargement will
cause an outpouching of the right heart contour.
Left Ventricle
Situated to the
left and posteriorly to the right ventricle.
Enlargement will
result on the PA-view in an increase of the heart size to the left and on the
lateral view in bulging of the lower posterior contour.
Right Ventricle
Most anterior
structure and is situated behind the sternum.
Enlargement will
result on the PA-view in an increase of the heart size to the left and can
finally result in the left heart border being formed by the right ventricle.
Left Atrium
The upper
posterior border of the heart is formed by the left atrium.
Enlargement will
result in bulging of the upper posterior contour
Left Ventricle
Forms the lower
posterior border.
Enlargement will
displace the contour more posteriorly.
Right Ventricle
The lower
retrosternal space is filled by the right ventricle.
Enlargement of the
right ventricle will result in more superior filling of this retrosternal
space.
Left Atrium enlargement

This is a patient with longstanding mitral valve disease and
mitral valve replacement.
Extreme dilatation of the left atrium has resulted in
bulging of the contours (blue and black arrows).
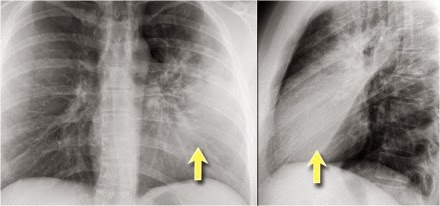
Right ventricle enlargement
First study the PA and lateral chest film and then continue
reading.
On these chest films the heart is extremely dilated.
Notice that it is especially the right ventricle that is
dilated. This is well seen on the lateral film (yellow arrow).
There is a small aortic knob (blue arrow), while the
pulmonary trunk and the right lower pulmonary artery are dilated.
All these findings are probably the result of a
left-to-right shunt with subsequent development of pulmonary hypertension.
The location of the cardiac valves
 is best determined on the
lateral radiograph.
is best determined on the
lateral radiograph.
A line is drawn on the lateral radiograph from the carina to
the cardiac apex.
The pulmonic and aortic valves generally sit above this line
and the tricuspid and mitral valves sit below this line .
On this lateral view you can get a good impression of the
enlargement of the left atrium.
Cardiac incisura

On the right side of the chest the lung will lie against the
anterior chest wall.
On the left however the inferior part of the lung may not
reach the anterior chest wall, since the heart or pericardial fat or effusion
is situated there.
This causes a density on the anteroinferior side on the
lateral view which can have many forms.
It is a normal finding, which can be seen on many chest
x-rays and should not be mistaken for pathology in the lingula or middle lobe.
The explanation for the cardiac incisura is seen on this
CT-image.

At the level of the inferior part of the heart we can
appreciate that the lower lobe of the right lung is seen more anteriorly
compared to the left lower lobe.
Pacemaker

There are different types of cardiac pacemakers.
Here we see a pacemaker with one lead in the right atrium
and another in the right ventricle.
A third lead is seen, which is guided through the coronary
sinus towards the left ventricle.
This is done in patients with asynchrone ventricular
contractions.
Pacing both ventricles at the same time will lead to
synchrone contractions and a better cardiac output.
Pericardial effusion

Whenever we encounter a large heart figure, we should always
be aware of the possibility of pericardial effusion simulating a large heart.
On the chest x-ray it looks as if this patient has a dilated
heart while on the CT it is clear, that it is the pericardial effusion that is
responsible for the enlarged heart figure.
Especially in patients who had recent cardiac surgery an
enlargement of the heart figure can indicate pericardial bleeding.
This patient had a change in the heart configuration and
pericardial bleeding was suspected.

Ultrasound demonstrated only a minimal pericardial effusion.
Continue with the CT.
There is a large pericardial effusion, which is located
posteriorly to the left ventricle (blue arrow).

The left ventricle id filled with contrast and is compressed
(red arrow).
At surgery a large hematoma in the posterior part of the
pericardium was found.
Notice that on the anterior side there is only a minimal
collection of pericardial fluid, which explains why the ultrasound examination
underestimated the amount of pericardial fluid.
Here another patient who had valve-replacement.

Notice the large heart size.
There is redistribution of the pulmonary vessels which
indicates heart failure.
Continue with the CT.

The CT-image shows a large pericardial effusion.
Always compare these post-operative chest films with the
pre-operative ones.
Calcifications

Detection of calcifications within the heart is quite
common.
The most common are coronary artery calcifications and valve
calcifications.
Here we see pericardial calcifications which can be
associated with constrictive pericarditis.
In this case there are calcifications that look like
pericardial calcifications,
 but these are myocardial calcifications in an
infarcted area of the left ventricle.
but these are myocardial calcifications in an
infarcted area of the left ventricle.
Notice that they follow the contour of the left ventricle.
Pericardial fatpad

Pericardial fat depositions are common.
Sometimes a large fat pad can be seen (figure).
Necrosis of the fat pad has pathologic features similar to
fat necrosis in epiploic appendagitis.
It is an uncommon benign condition, that manifests as acute
pleuritic chest pain in previously healthy persons.
Pericardial cyst

Pericardial cysts are connected to the pericardium and usually contain clear fluid.
The majority of pericardial cysts arise in the anterior
cardiophrenic angle, more frequently on the rightside, but they can be seen as
high as the pericardial recesses at the level of the proximal aorta and
pulmonary arteries .
Most patients are asymptomatic.
On the chest x-ray it seems as if there is a elevated left
hemidiaphragm.
On CT however there is a cyst connected to the pericardium
suggested reading