Pulmonary Medicine Blog By Dr Deepu.
Lung Cancer incidence is on rise so does the metastasis to the
lungs. As the age increases the incidence of lung cancer and also the lung
metastasis increases.
An elderly male presented to us with weakness and giddiness associated with chest pain since a month. Clinical examination revealed an enlarged right supraclavicular node. Rest of the clinical findings were normal.
BUY ONE OF THE BEST BOOKS FOR CHEST RADIOLOGY! PRICES SLASHED WITH INDIAN EDITION
BUY ONE OF THE BEST BOOKS FOR CHEST RADIOLOGY! PRICES SLASHED WITH INDIAN EDITION
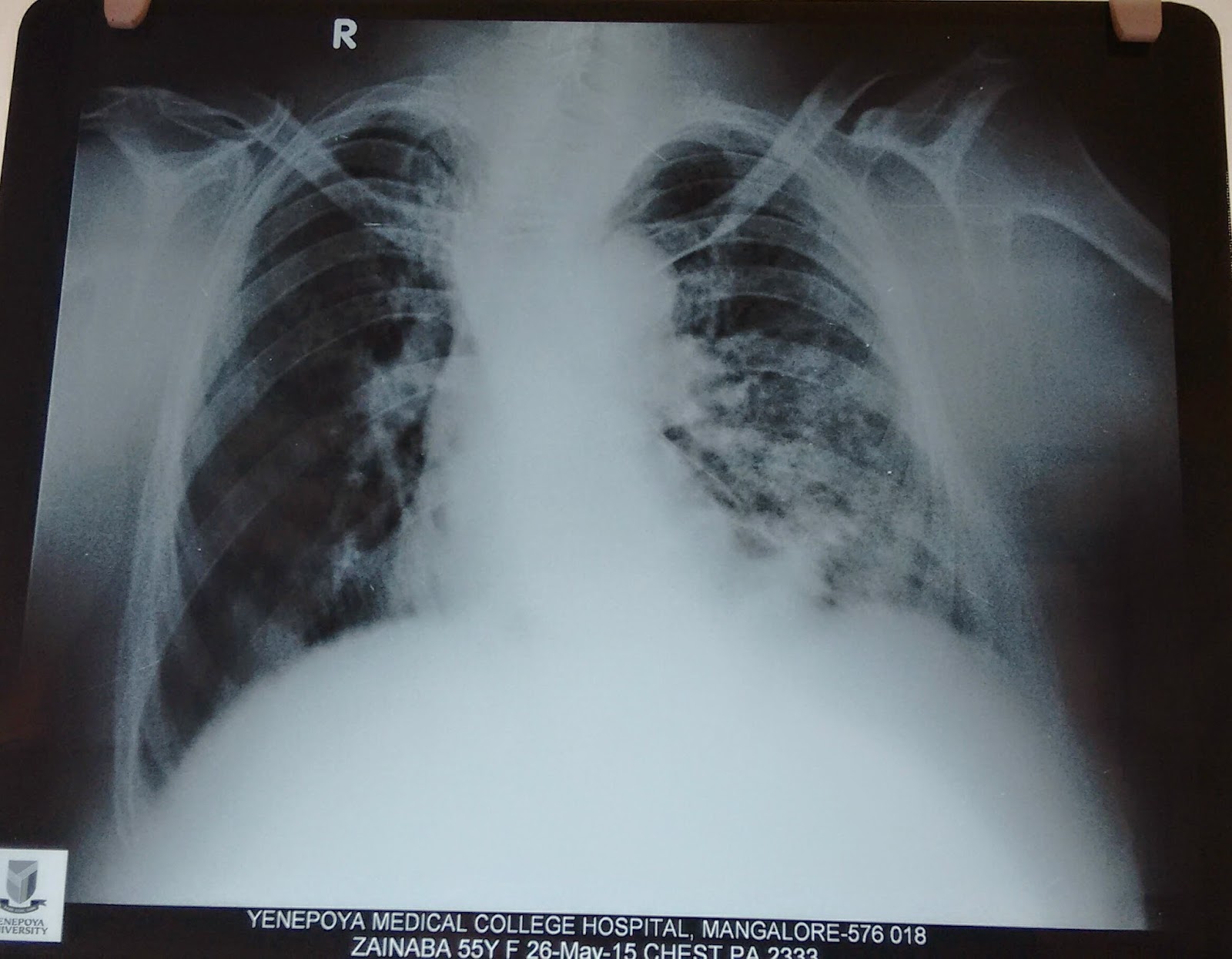
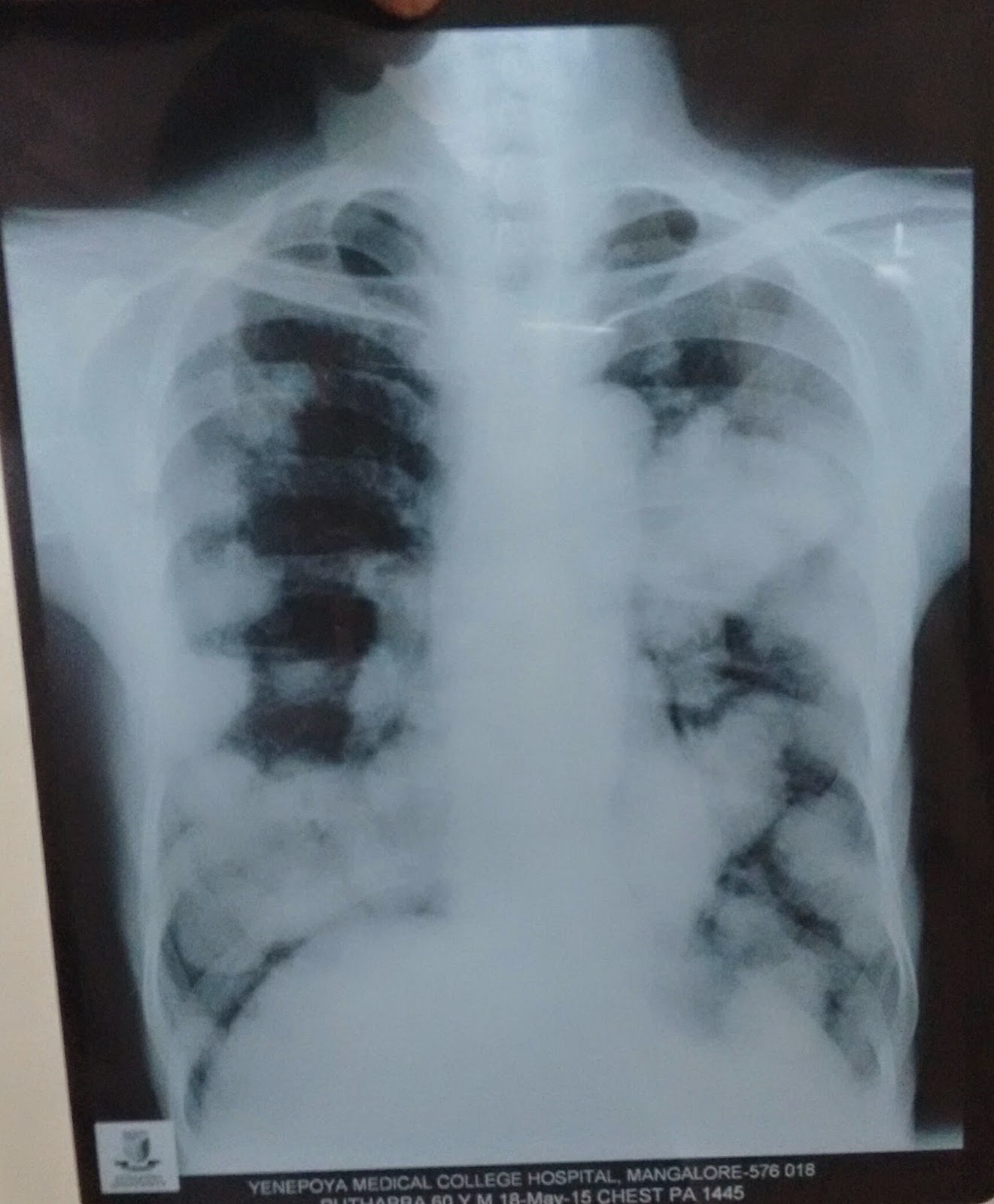
Before proceeding study this chest X Ray carefully.

Chest X ray shows large , well circumscribed, round pulmonary nodules that are distributed in upper mid and lower lung zones bilaterally, some forming into a mass but most of them are seen concentrated in the lower zones and mostly along the peripheral lung fields. also there is a homogenous mass in the left mid zone just lateral to the descending aorta. The diagnosis could be cannon ball secondaries with unknown primary.
Study the CT images before proceeding


The CT scan above shows multiple nodules of varying sizes, concentrated mostly in the lower lobes and left upper lobe bronchus seems occluded partially by the mass. Here study this mediastinal window and coronal cuts


We screened his brain , GIT, bones and Genitourinary system for primary Tumor, the scans were normal , further we considered bronchoscopy and Scopy showed a fungating mass in the left upper lobe, Biopsy reports are awaited. Will update once it becomes available.
Cannonball metastases are large, well
circumscribed, round pulmonary
metastases that appear, well, like cannonballs.



The French term "envolée de ballons"
which translates to "balloons release" is also used to describe this
same appearance.


Causes of Cannon Ball
Metastais
Classical- renal cell
carcinoma choriocarcinoma,
Less commonly - prostate
cancer, synovial sarcoma or endometrial
carcinoma.
Pulmonary metastases are
very common and it is due to metastatic
spread to the lungs from a variety of tumour. It can spread via
blood or lymphatics.
Clinical presentation
Pulmonary metastases are asymptomatic usually,
The constitutional symptoms are related to primary cancerous
metastatic condition
Those attributable to the primary tumour dominating.
Haemoptysis , Chest pain , difficulty
in breathing and pneumothorax are sometimes the
presenting symptom.
Pathology
Tumour cells reach the lungs via the pulmonary circulation,
where they lodge in small distal vessels.
The most common primaries to result in pulmonary metastases
include:
breast carcinoma
colorectal carcinoma
renal cell carcinoma
uterine leiomyosarcoma
head and neck squamous cell carcinoma
Primaries which most frequently metastasise to lungs
(although in themselves much less common tumours) include:
choriocarcinoma
Ewing sarcoma
malignant melanoma
osteosarcoma
testicular tumours
thyroid carcinoma
Radiographic features
Pulmonary metastases characteristically appear as
peripheral, rounded nodules of variable size, scattered throughout both
lungs . uncommon features include consolidation, cavitation, calcification,
haemorrhage and secondary pneumothorax.
HERE IS A SMALL BUT QUITE INFORMATIVE BOOK ON CHEST X RAY DOCTORS SHOULD READ.
HERE IS A SMALL BUT QUITE INFORMATIVE BOOK ON CHEST X RAY DOCTORS SHOULD READ.
Plain radiograph
Plain films are insensitive, although frequently able to
make the diagnosis, as often pulmonary metastases are large and numerous.
CT
CT is excellent at visualising pulmonary nodules. Typically
metastases appear of soft tissue attenuation, well circumscribed rounded
lesions, more often in the periphery of the lung. They are usually of variable
size, a feature which is of some use in distinguishing them from a granuloma.
A prominent pulmonary vessel has frequently been noted heading
into a metastasis. This is termed the feeding vessel sign.
Some tumours have a predilection for innumerable small
metastases (miliary pattern):
Malignant melanoma
Osteosarcoma
Renal cell carcinoma
Thyroid carcinoma
Trophoblastic disease( choriocarcinoma)
Pulmonary metastasis may be single. Seen most frequently in colorectal carcinoma.
Other primaries which often present with solitary metastases
include:
Malignant melanoma
skeletal sarcoma
adenocarcinomas in general
Adenocarcinoma metastases may rather than displace or
destroy adjacent lung parenchyma, cells grow in a lepidic fashion (spread along
aleveolar walls) resulting in pneumonia-like consolidation. Air
bronchograms may also be visible.
Cavitation is present in ~4% of cases. The most common
primary is squamous cell carcinoma, most often from the head and neck or from
the lung. Other primaries include adenocarcinomas, and sarcomas.
Calcification, although uncommon and more frequently a
feature of benign aetiology (e.g. granuloma or hamartoma) is also seen with
metastases, particularly those from papillary thyroid carcinoma and
adenocarcinomas. Treated metastases, osteosarcomas and chondrosarcomas may also
contain calcific densities.
A halo of ground-glass opacity representing
haemorrhage can be seen, particularly surrounding haemorrhagic pulmonary metastases, such as choriocarcinoma and angiosarcoma.
Treatment and prognosis
In general presence of pulmonary metastases is an ominous
finding, indicating poor prognosis. The specific prognosis will however depend
on the primary tumour.
Complications
Tumours with prominent necrosis located near a pleural
surface may result in a pneumothorax. Osteosarcoma is
classically described as the pulmonary metastasis that results in pneumothorax.
Another cause of pneumothoraces include cystic or cavitatory pulmonary
metastases.