Pulmonary Medicine Blog By Dr Deepu


There are a few things which
beginners often miss in a chest x ray, one among those is failure to comment on
the diaphragms.
Today I am going to discuss
importance of tracing diaphragm in a chest X ray with an example.
Normal diaphragm in a chest X ray has
the following characteristics


1. Trace
the diaphragm on right and left
2. The right
diaphragm is usually placed between the fifth and the sixth Rib in the mid
clavicular line, It can be seen upto middle of sixth and seventh rib.
3. The
Diaphragms are usually not at the same level on the frontal , erect ,
inspiratory chest X rays, but they are usually within one rib intercostals space
height ( roughly 2 cm) of each other.
4. The
left diaphragm is usually lower than right.
5. The
costophrenic angles should be sharp, making an acute angle.
6. If the left hemidiaphragm is equal to Right or
higher than Right or Right diaphragm is higher than left by more than 3 cms,
Causes of diaphragmatic elevation should be considered.
The causes of elevated hemidiaphragm are
1.
Causes above the diaphragm- decreased lung
volume due to Lung Collapse, lobectomy, pneumonectomy , fibrosis and pulmonary
Hypoplasia
2.
Causes in the diaphragm- Phrenic nerve palsy ,
diaphragmatic evantration
3.
Causes below the diaphragm- abdominal
malignancy, subphrenic abscess, distended hollow
viscus.
After knowing the cause I want to discuss
with you a chest x ray where the subtle change in the diaphragm was missed.
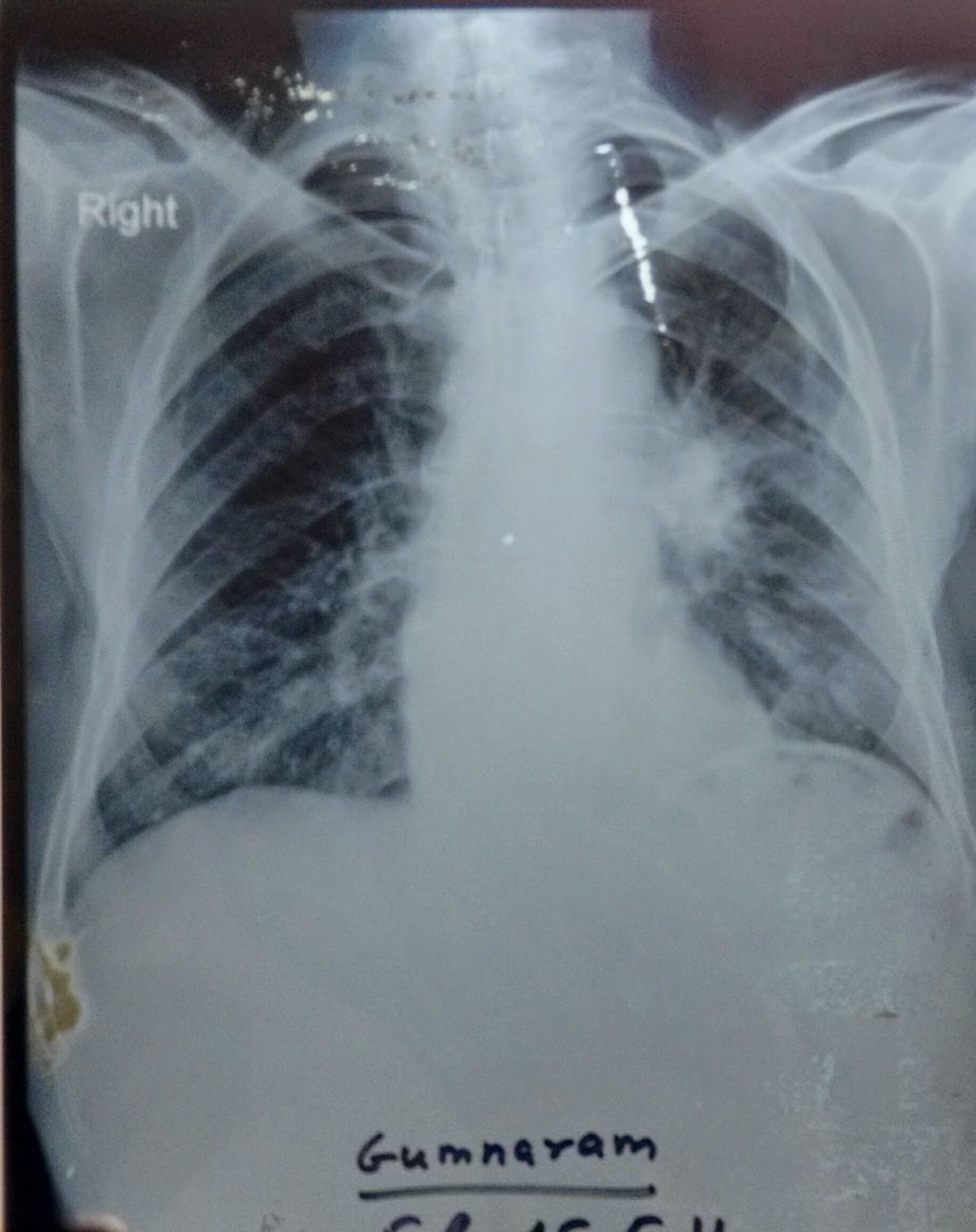
Before we proceed Read the chest X ray
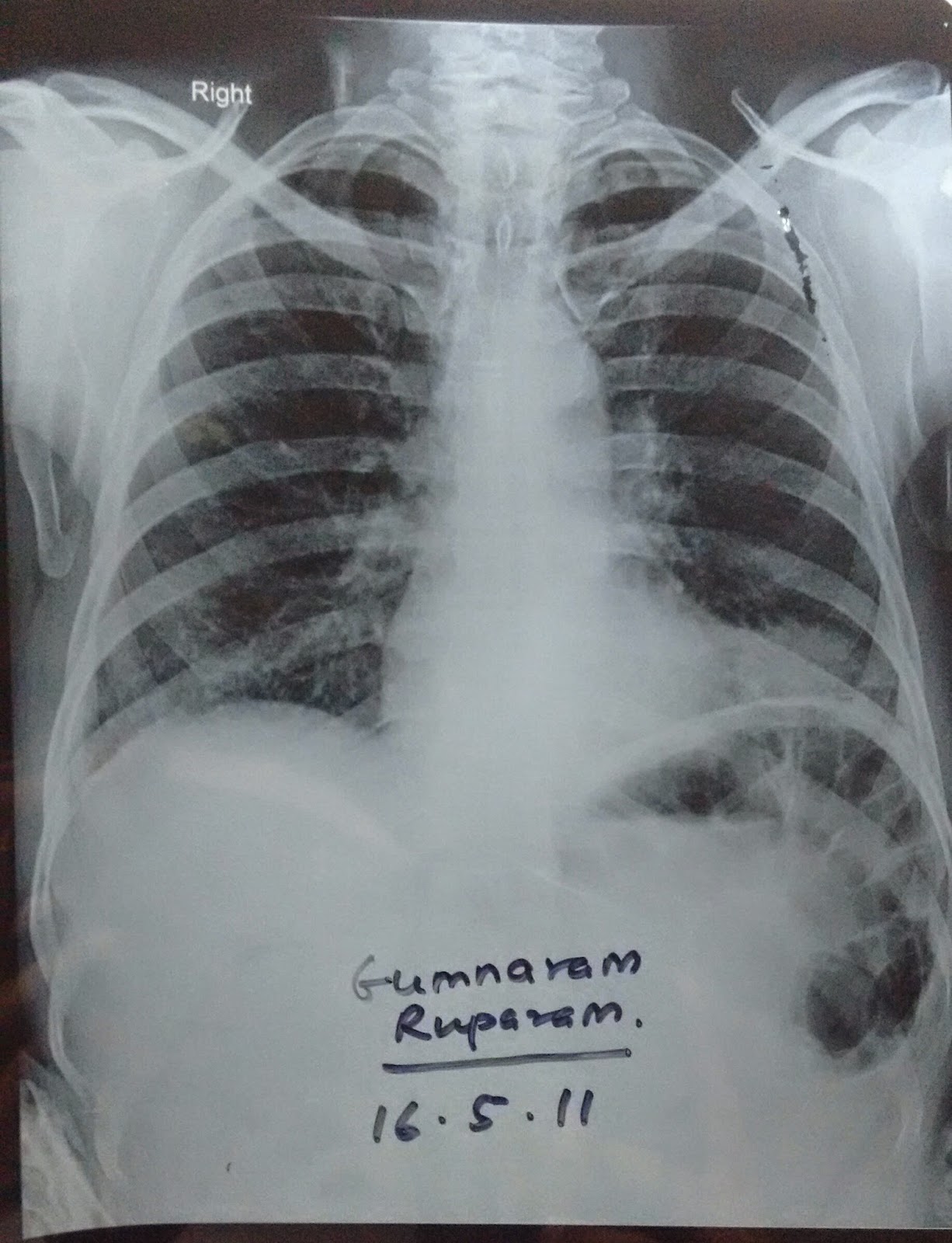
The Chest X ray showed a subtle change in Diaphragm
1. Both the diaphragms are at the same levels.
2. The air shadow underneath the left diaphragm is more prominent.
3. The patient was not evaluated further because chest X Ray appeared normal and sent home with conservative treatment for COPD.
He came back to our center with hemoptysis one month later referred from the center which treated him initially, a second Radiograph was performed. study the Chest X Ray before proceeding further.
The chest X ray now shows features of full blown disease, the hilum is prominent with CORONA RADIATA SIGN suggestive of bronchogenic carcinoma, The left Diaphragm is now placed higher compared to right. Further HR and CECT revealed a tumor in the Left Main bronchus with lymph node metastasis. With Bronchoscopy the diagnosis of squamous cell carcinoma was made.
With this I will end this post, requesting everyone to look at any subtle changes in diaphragm which if ignored may cause some grave diagnosis at a later date.